
From The New York Times Disunion, "The Minister of Death," by Carole Emberton, on 17 August 17 2012 -- From April 29 to May 30, 1862, some 300,000 men — including my great-great grandfather, Pvt. Edward Willis — converged at the tiny railroad depot of Corinth, in northern Mississippi, where they laid siege to the Confederate forces under Gen. P.G.T. Beauregard. The Union soldiers scarred the landscape with miles of earthen fortifications. But the trenches could not protect Edward and his fellow soldiers from what Thomas Macaulay called “the most terrible of all the ministers of death,” a predator that craved those close, confined spaces, where men’s blood, breath and spit mingled freely. Although they fought on opposite sides of the trenches, the Union and Confederate forces shared a common enemy: smallpox.
Edward was hospitalized for the two months following the Union’s capture of Corinth. While his service record gives no reason for his hospitalization, his wife Edith’s pension application after his death in 1878 claimed that he had contracted smallpox while in the Army, “which afflicted his eyes and head, from which condition said soldier never recovered.” It is likely that he spent June and July in a “pest house,” quarantined along with other soldiers displaying signs of what Army doctors called “eruptive fevers” – smallpox, scarlet fever, measles and erysipelas (a bacterial skin infection caused by streptococcus).

Of these infectious diseases, smallpox was not the most common, but it was the most feared. During the course of the war, the Union Army reported only about 12,000 cases of smallpox among white troops, compared to nearly 68,000 cases of measles. However, total deaths from both diseases were about the same — 4,700 and 4,200, respectively — with the death rate from smallpox hovering around 39 percent.
It is little wonder that medical personnel in both armies wrung their hands over the prospect of an impending smallpox epidemic, scouring Northern cities and the Southern countryside in search of small children to inoculate so that their scabs could be harvested to produce “pure vaccine” free from other diseases, like syphilis, that might be transmitted from adults. Fear of the “speckled monster” also led soldiers to take desperate measures, including self-inoculation with the pus from other men’s sores that they believed to be smallpox but could, in fact, be syphilis or some other gangrenous lesion. The resulting infections incapacitated thousands of soldiers for weeks and sometimes months. The inspector general for the Army of Northern Virginia estimated that when the battle of Chancellorsville was fought in May 1863, as many as 5,000 men were unfit for duty due to these “spurious vaccinations.”

It is widely accepted that disease claimed more lives than bullets during the Civil War. The first wave of infection hit new recruits soon after they arrived in camp. Men from rural areas were especially vulnerable, lacking immunity to the childhood diseases to which their urban counterparts most likely had been exposed. Before Edward’s regiment, the 17th Kentucky, left camp at Calhoun where they enrolled, an outbreak of measles “raged through the camp like some attacking army.” According to the unit’s historian, more than 20 men died in those first few months, before they even heard a rebel gun.
Historians of medicine commonly refer to the mid-19th century as the “medical Middle Ages” in the United States because of the lack of understanding about sanitation and contagion, and thanks to a medical profession that lagged behind its European counterparts in procedural knowledge, institutional structure and numbers of certified physicians. When the war began, the Union Army medical division consisted of fewer than 100 surgeons and assistant surgeons. There was no organized ambulance service to remove wounded soldiers from the battlefield, and those who did make it to a squalid camp hospital fared little better than those left to die where they fell. With the help of the United States Sanitary Commission and a reorganization of the Army medical corps, which included the creation of an ambulance corps to rival any European army and a modern general hospital system across the nation, the Civil War revolutionized medical care in the United States. But for those men who fell victim to smallpox and other infectious diseases, modernity mattered little.

Smallpox was an ancient disease. For millenniums, it had followed the routes of trade, empire and war. The earliest descriptions of smallpox’s telltale pustules date from the fourth century A.D. in China. However, scientists believe they have identified smallpox scars on the bodies of Egyptian mummies from the 12th century B.C. “An inveterate camp follower,” according to the historian Michael Willrich, the virus, whose Latin name variola means “spotted,” spread across the globe along with the armies of the Roman, Mongol and Ottoman Empires, claiming the lives of kings, queens and emperors as well as common folk. No one was safe. It followed Europeans to the “New World,” wiping out as much as 90 percent of the indigenous populations of North and South America and the Caribbean. By the time the English physician Edward Jenner introduced the first vaccine for smallpox in 1798, at least 400,000 Europeans were dying each year from the disease.
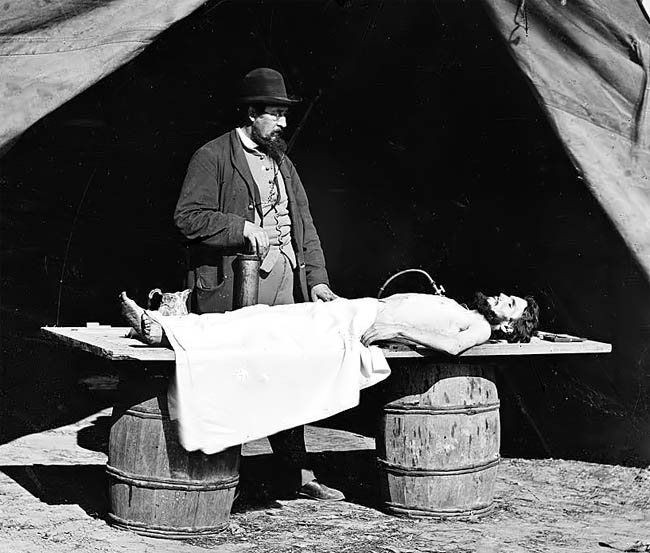
What made smallpox so deadly? W.W. Brown, a surgeon with the 7th New Hampshire stationed in St. Augustine, Fla., wrote that the disease, “when uncomplicated, requires no medication except an occasional anodyne to allay nervous irritation and procure rest.” Unfortunately, in an era before modern sanitation or antibiotics, not to mention in the middle of a war, few cases were “uncomplicated.” Many of the men stricken with smallpox were already suffering from other ailments – fatigue, malnutrition, typhoid or dysentery. With their immune systems compromised, smallpox struck a deadly blow. In the worst cases of “fulminating and malignant” smallpox, the patient began to bleed out through the mucus membranes and the skin sloughed off in great patches. The virus attacked the internal organs, resulting in “general toxemia” and eventual death. Post-mortem examinations revealed considerable tissue deterioration and severe internal hemorrhaging.

The case of 25-year-old Enos W. Bratcher of the Third Kentucky Cavalry was typical. Bratcher contracted smallpox while in the hospital near Madison, Ind., being treated for tonsillitis. Although the doctors noted that “his general health appeared good,” he also suffered from chronic diarrhea. As with other smallpox patients, doctors treated Bratcher’s sores with a tincture of iodine applied with a small brush to his face, where the pustules congregated and ran together. For pain, he was given the ubiquitous “Dover’s powders,” a crystallized combination of ipecac and morphine dissolved in liquid. He was encouraged to drink fluids, although the prescribed mix of “ale, milk-punch, egg-nog, chicken and beef tea” probably did not appeal to a man suffering from violent nausea. In other cases, when the oozing pustules invaded the mouth and throat, making it difficult for the sufferer to breathe or swallow, doctors gave a small dose of potassium chlorate as a gargle, a solution that could prove fatal if swallowed. In any case, nothing worked for Bratcher. Delirious with fever and with his tongue and teeth turned black, a common occurrence in patients suffering from dehydration and prolonged infection, he died after two weeks of hellish suffering.
For those like Edward, who survived smallpox, the road to recovery could be long. In addition to the pockmarks left on the skin, the disease could cause permanent hair loss, recurring eczema and deformities in limbs resulting from muscle and tissue damage. In men, it could result in sterility. The virus infected the eyes, causing eruptions on the eyelids and scarring of the cornea (the eye problems cited in Edith Willis’s pension application were consistent with the long-term effects of smallpox).
There were psychological effects as well. Walt Whitman may have admired “faces pitted with small-pox over all latherers,” but not everyone saw the scars as symbols of rugged masculinity. Instead, the disease’s association with filth, vagrancy and foreignness could stigmatize survivors long after their bodies had recovered, condemning them to social ostracism and loss of employment.
The racial politics of disease in the era of emancipation also complicated the cultural understanding of smallpox. After multiple epidemics among freed people, smallpox assumed a negative association with blackness, further adding to the popular belief that sufferers were both filthy and inferior. But if black soldiers and freed people suffered from smallpox disproportionately, it wasn’t because they were inherently susceptible to it because of their race. As the historian Jim Downs points out in his recent book on the health care of former slaves, smallpox spread among the freed population because of unsanitary living conditions, including the refusal of local officials to properly bury the dead and burn their belongings, which carried the contagion. Already malnourished and in poor health, many of the slaves flocking to Union lines and joining the ranks of the Federal Army stood little chance against the disease.
Other than his eye problems, I do not know what other scars Edward bore from his battle with smallpox. He had faced down an enemy much older, and in the grand scheme of things far deadlier, than the Confederacy. But there were no medals earned from his victory. By August 1862, he was back on duty, driving the commissary wagon. (source: The New York Times)
No comments:
Post a Comment